- The Foundation
- Aims
- Research Activities
- News
- FOUNDATIONCONTACT
- SCIENTIFIC ACTIVITYPublications
- Studies
- Score Calculators
BARCELONA—The basis of genetic ancestry (and race) underlying differences in disease occurrence, outcomes or response to treatment remains unclear and most often racial and ethnic diversity is underrepresented in clinical research contributing to further expand the gap of health inequities. According to the Global Burden of Disease 2010 study, complications of cirrhosis accounted for 1 million deaths worldwide and caused 31 million disability adjusted life years (DALYs) that year. Noteworthy, liver cirrhosis mortality in Mexico was the highest in Latin America in 2010 with a mortality rate of 38.3 per 100,000. Patients with acute decompensation of cirrhosis suddenly develop ascites, hepatic encephalopathy, gastrointestinal hemorrhage, or any combination thereof. The CANONIC study, the first large, observational study carried out in Europe by the European Association for the Study of the Liver-Chronic Liver Failure (EASL-CLIF) Consortium, identified acute-on-chronic liver failure (ACLF) as a distinct syndrome that develops in 30% of patients with acute decompensation of cirrhosis, and is characterized by acute systemic inflammation, multi-system organ failure, and a high risk of death within 28 days after hospital admission. The ACLARA study – Prevalence, epidemiology, characterization and mechanism of ACLF in Latin America – sheds new light on the potential impact of genetic ancestry and reported race on the severity of ACLF and risk of short-term mortality. The study carried out in 1274 patients non-electively hospitalized for acute decompensation of cirrhosis in 44 university hospitals from 27 cities in 7 Latin American countries (Argentina, Brazil, Chile, Colombia, Mexico, Paraguay, and Peru), highlights the importance of including genetic ancestry (and race) in liver disease research and clinical practice for being variables that capture relevant epidemiological information. Findings from this study, published ahead of print in Gastroenterology, show that social factors (i.e., admission to public hospitals compared to private hospitals) and markers of organ function independently correlate with higher short-term mortality. The data also suggest an association between increased percentage of Native American ancestry (and reported race) and development of ACLF independent of alcohol-related hepatitis and bacterial infections, two major precipitant events of acute decompensation of cirrhosis and progression to ACLF.
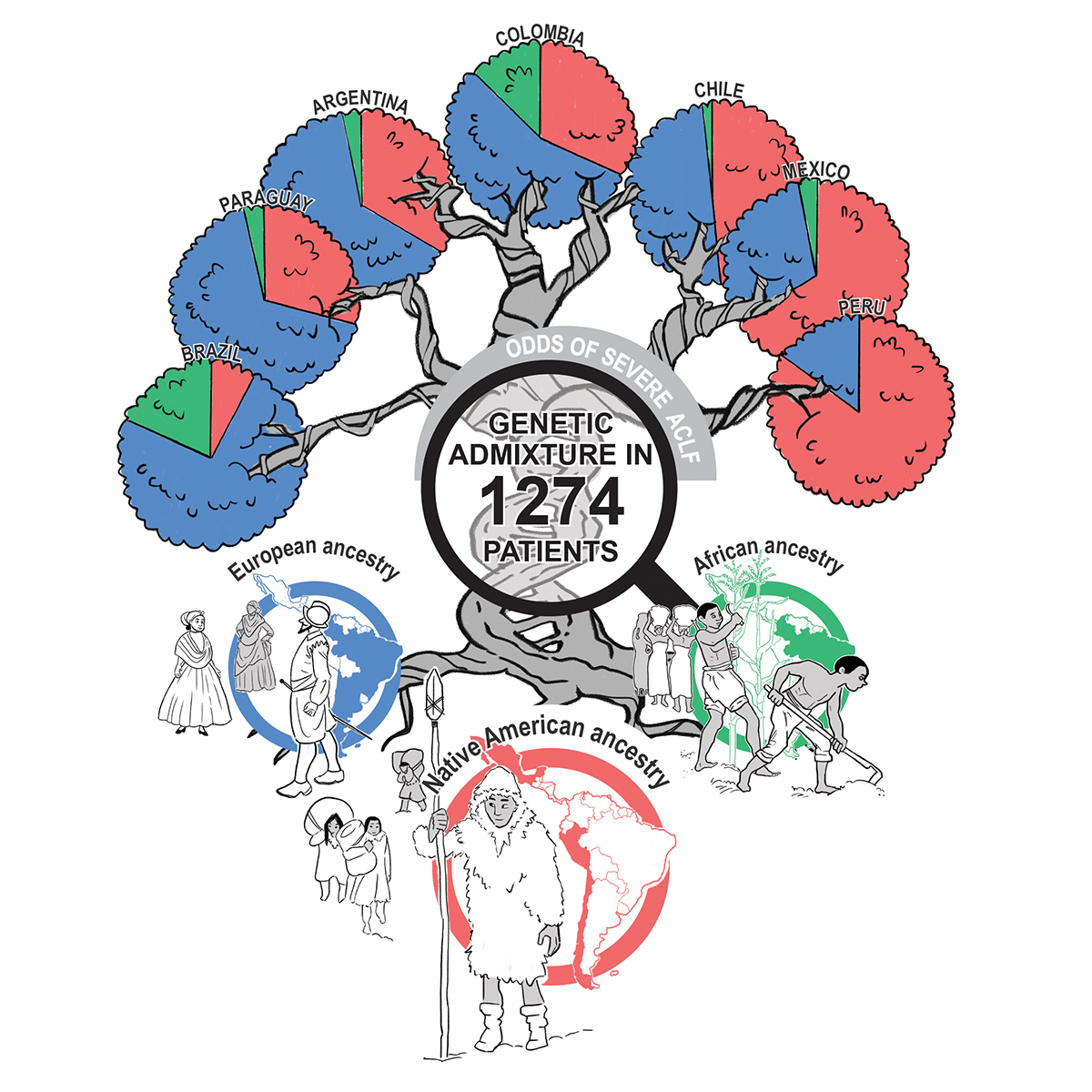
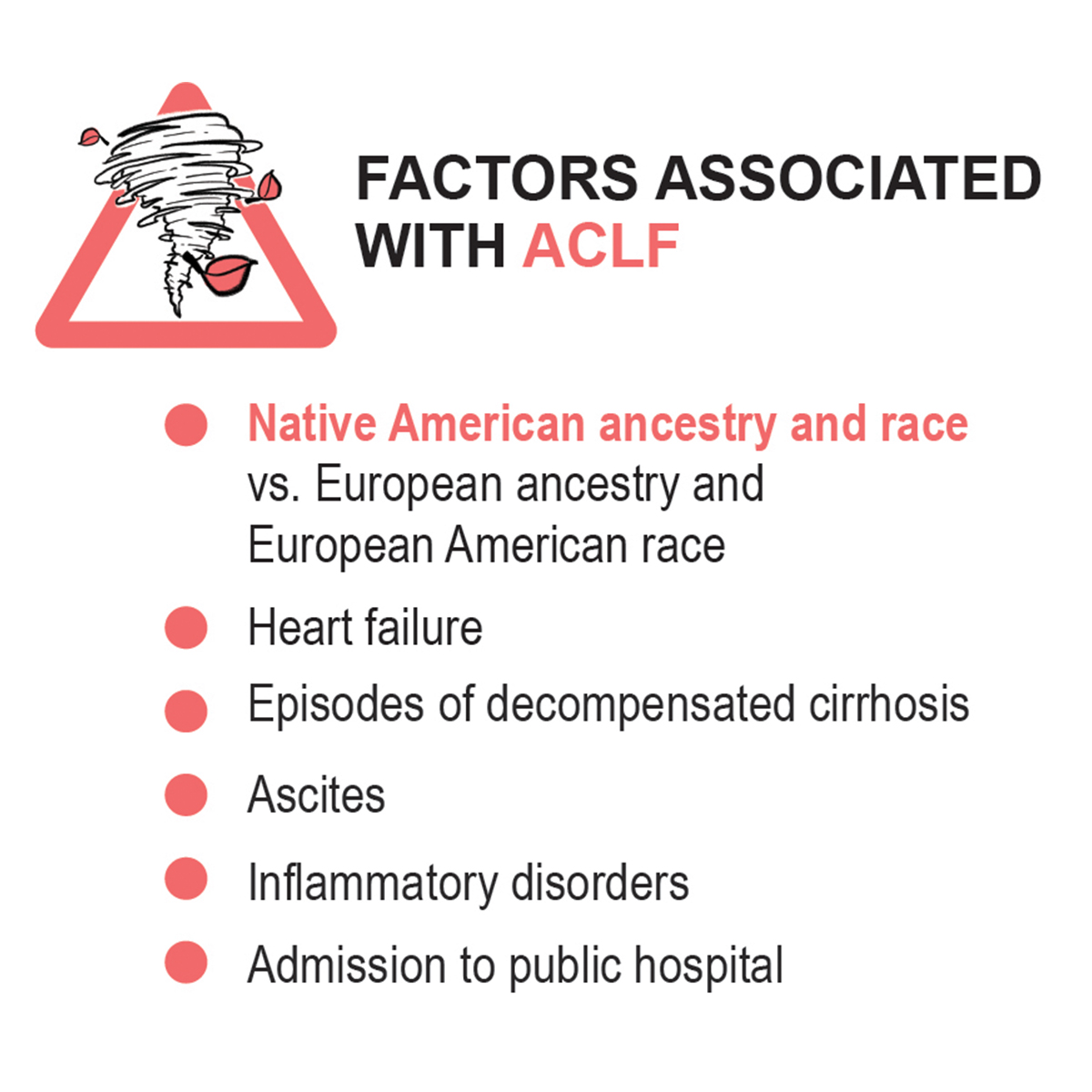
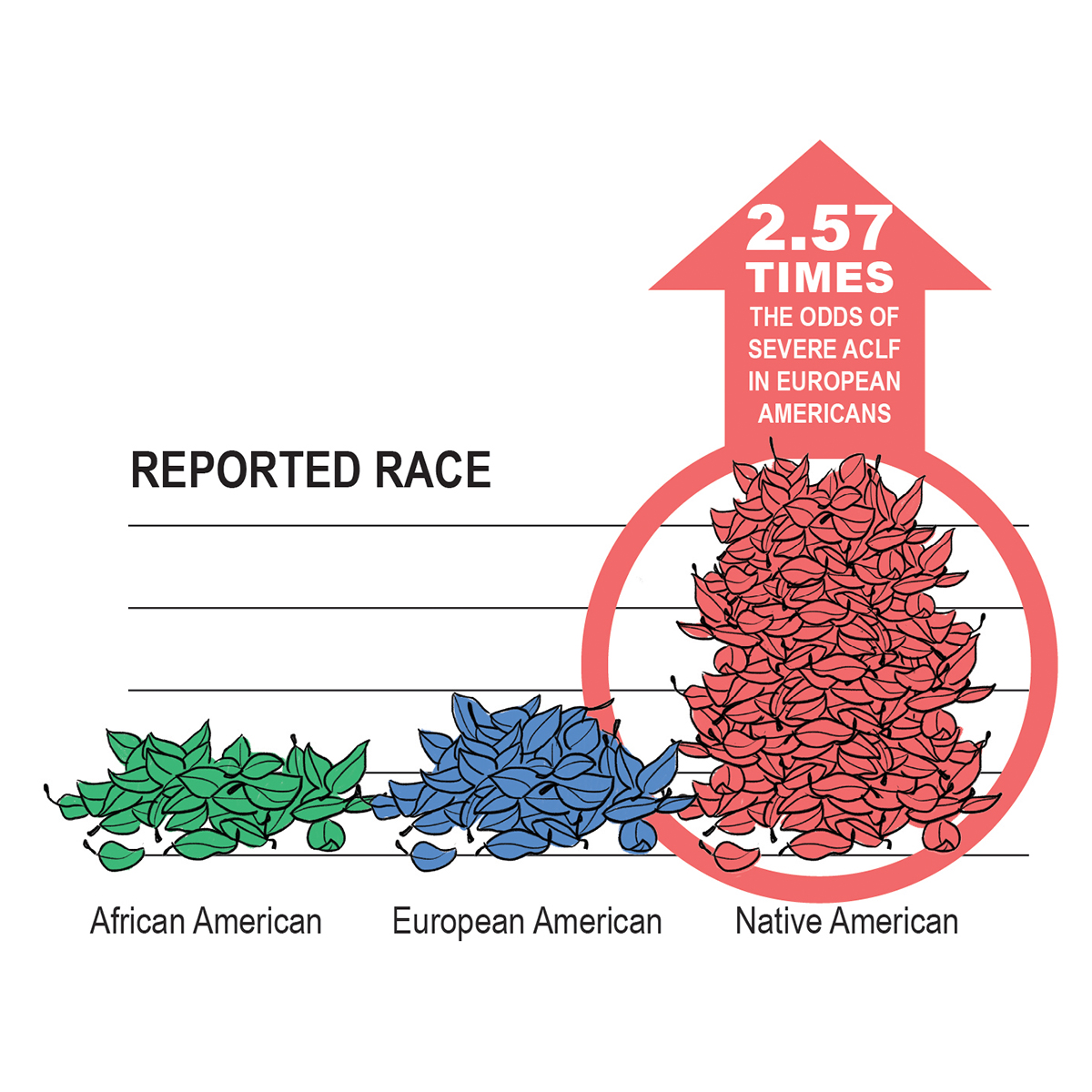
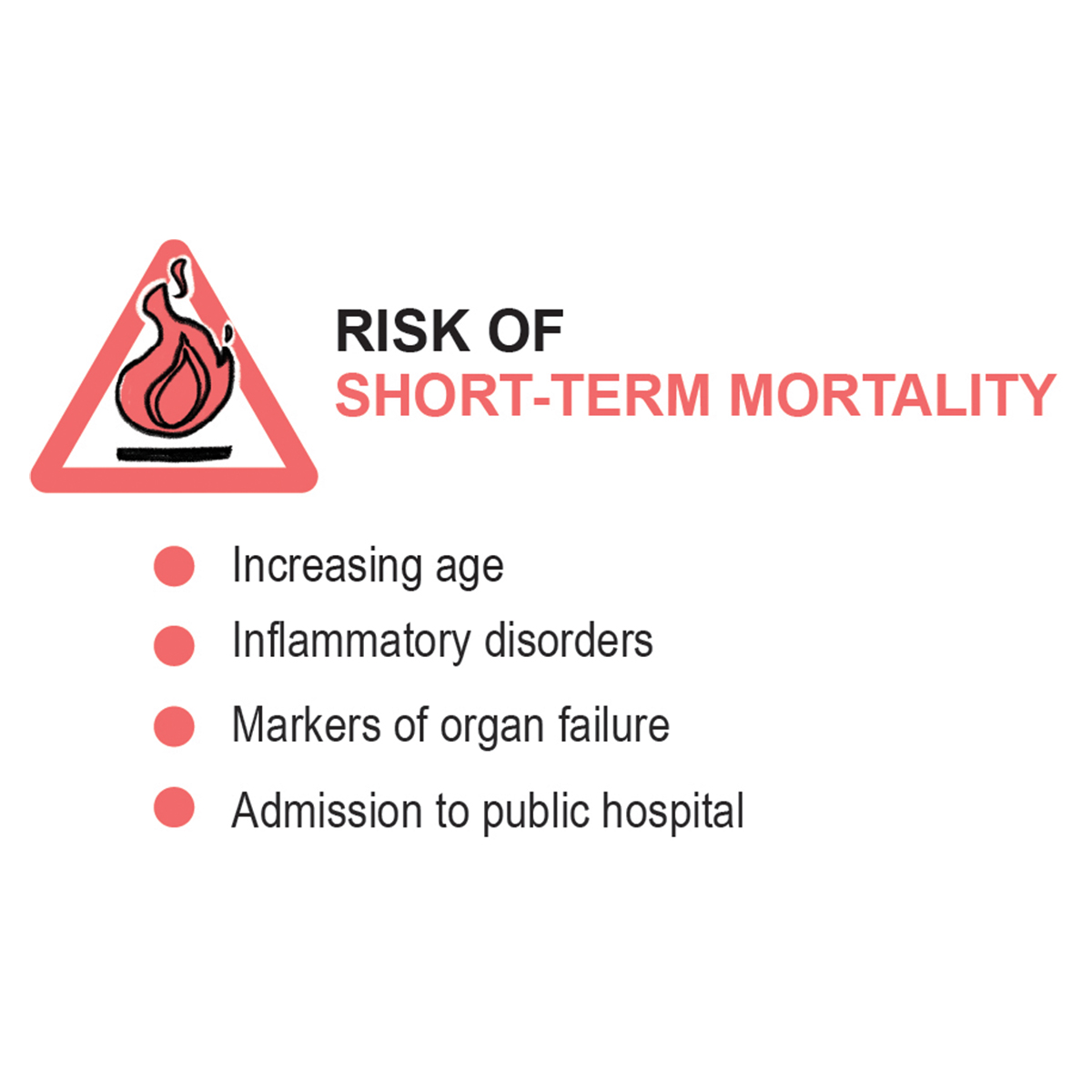
Image: © European Foundation for the Study of Chronic Liver Failure.
Populations across Latin America today show differing patterns of percentages of genetic variants of Native American, African and European ancestry as a result of a long history of modern human migrations and admixture (i.e., genetic exchange among people of different descent). In an effort to gain further insight into the relationship between genetic ancestry, race and probability of developing ACLF and associated risk of short-term mortality in the admixed Latin American populations, researchers looked at hospitalized patients with acute decompensation of cirrhosis from Argentina, Brazil, Chile, Colombia, Mexico, Paraguay, and Peru.
“In 2013, the CANONIC study provided the definition, diagnostic criteria, information on the clinical course and prognosis of a new syndrome called ACLF. However, it was performed only in Europe. Investigating ACLF in other cohorts may strengthen the understanding of other upstream factors on disease expression. The Latin American region, with different racial and genetic ancestries, is a unique landscape for in-depth assessment of such factors”, says first co-author in the paper Alberto Farias, Principal Investigator at Hospital das Clínicas, University of São Paulo School of Medicine, Brazil.
Reserchers genotyped 529,687 single-nucleotide polymorphisms and assessed genetic ancestry with the use of autosomal markers of ancestry, and not by parental indicators of ancestry. "Y-single nucleotide polymorphisms and mitochondrial DNA could provide a limited characterization of the genetic admixture of a given population", explains Richard Moreau, co-lead investigator of the study and Principal Investigator at EF CLIF, Spain. In addition to genetic ancestry, race was assessed by the physician at hospital admission. "We decided to assess race reported by the attending physician and not self-reported race because we expected to have a substantial number of patients with hepatic encephalopathy who would not be able to report race. In their daily practice, Latin American investigators are used to assessing race based on phenotypic characteristics. In this study, we found an excellent correlation between the reported Native American race and the percentage of Native American genetic ancestry", adds Moreau.
The ACLARA study group reported ACLF of any grade in 31.0% of patients at enrollment, of these 54.2% were presented with ACLF grade 1, 24.9% had ACLF grade 2, and 20.9% had ACLF grade 3 (i.e., three or more organ failures). Overall, patients admitted to hospital with ACLF showed higher percentage of Native American ancestry and lower percentage of European ancestry compared to patients with acute decompensation of cirrhosis without ACLF (22.6% and 53.4% vs. 12.9% and 59.6%, respectively). The percentage of African ancestry was low in both hospitalized patients with ACLF and patients without ACLF among participating countries (6.9% vs. 6.5%).
Researchers collected a series of sociodemographic and clinical characteristics of patients with acute decompensation of cirrhosis admitted to hospital to build multivariable models to predict the likelihood of developing ACLF and risk of 28-day mortality based on differences in percentage of genetic ancestry or reported race. Taking the variables separately in univariate analyses, diabetes, the most common comorbidity of cirrhosis in this cohort, was found to be positively associated with ACLF. Non-alcoholic fatty disease as a cause of cirrhosis and prior treatment with biguanides – oral diabetes medication indicated to help lower the production of glucose in the liver and prevent insulin resistance, were not included in multivariable models for ACLF due to the strong correlation of these variables with diabetes in an attempt to eliminate potential confounders. Chronic kidney disease not requiring hemodialysis was also excluded, as increased level of creatinine is a criterion for the presence of ACLF. Researchers found that a 10% increase in the percentage of Native American ancestry was associated with an 8% increase in the risk of developing ACLF, while reported Native American race resulted in an increase of the likelihood of presenting ACLF by 2.57 times the probability of ACLF in patients reported as European American.
Factors that appeared to be linked to presentation of ACLF at enrollment included heart failure, episodes of decompensated cirrhosis within 3 months prior to enrollment in the study, referral from another hospital, enrollment with bacterial infection and sepsis, alcohol-related hepatitis, or ascites. On the contrary, gastrointestinal hemorrhage was associated with lower odds of developing ACLF.
Researchers also used univariate analyses to identify factors associated with liver transplant-free survival within 28 days after enrollment to build a second model to predict short-term mortality. In this context, the concentration of serum bilirubin – a biomarker of liver function – although associated with short-term mortality, strongly correlated with international normalized ratio and, thus, was excluded from subsequent multivariable analyses. While in univariate analyses both genetic ancestry and race were associated with short-term mortality, in multivariable analyses, neither genetic ancestry nor race appeared to be associated with risk of death within 28 days. Only when organ function-related variables were excluded, both percentage of genetic ancestry and race correlated with short-term mortality.
"A meticulous data collection and rigorous analysis is required to gather the complex relationships between variables. Univariate analysis focuses on a single variable at a time, offering a straightforward approach. It is easier to implement, but it may overlook potential confounding factors. Whereas, multivariate analysis considers multiple variables simultaneously, providing a more comprehensive understanding of complex relationships yielding a more holistic perspective. However, it requires sophisticated modelling techniques, specially to avoid overfitting/underfitting the data and the interpretation is intricate", says Anna Curto Vilalta, co-first author in the paper and former bioinformatician at EF CLIF, Spain.
Variables associated with higher 28-day mortality included increasing age, admission to public hospital (vs. private hospital), and enrollment with bacterial infection and sepsis, or alcohol-related hepatitis. Clinical data and laboratory measurements including lower arterial pressure or lower SpO2 to FiO2 ratio, higher level of creatinine in blood or international normalized ratio, lower levels of albumin in blood, or higher white blood cell count, were also associated with higher 28-day mortality. The only social factor independently associated with higher short-term mortality was admission to public hospital. The majority of patients admitted to public hospitals were younger, with low socioeconomical status and low educational attainment. Both Native Americans and African Americans were overrepresented among these patients that showed higher percentage of Native American and African ancestries and lower European ancestry. Compared with patients admitted to private hospitals, a higher percentage of patients admitted to public hospitals died without receiving liver transplantation within 28 days of hospitalization (14.8% vs. 20.5%), and the percentage of patients enrolled with severe ACLF (i.e., ACLF grades 2 or 3) that received liver transplantation was lower in public hospitals compared to private hospitals (9.1% vs. 25.0%). Moreover, 26.8% of Native Americans were presented with ACLF grades 2 or 3, while only 8.1% of African American and 10.3% of European American patients were admitted to hospital with severe ACLF. A higher percentatge of Native American patients died within 28 days after hospitalization comparted to African American and European American patients (28.5% vs. 15.0% and 17.3%, respectively).
"The most striking novel finding of this study was that Native American genetic ancestry or Native American race (vs. European American race) were independently associated with ACLF at presentation, finding that indicates differences in genetic ancestry or race contribute to outcome disparities in cirrhosis", says Moreau. "The association of Native American genetic ancestry and Native American race with ACLF indicate that Native American patients with cirrhosis should be included in programs of tight surveillance in order to benefit from urgent treatment of triggers of complications of cirrhosis. This could be first step towards precision medicine, which is an unmet medical need in the field of decompensated cirrhosis. In addition, the discovery that differences in genetic ancestry and race are associated with differences in outcomes among patients with acute decompensation of cirrhosis, may change the policy of prioritization and allocation of liver transplants relative to other patients with similar MELD (model for end-stage liver disease) score", adds Moreau.
Moreau who was Principal Investigator in the CANONIC study and also contributed to the investigation of the largest cohort of patients hospitalized with decompensated cirrhosis yet analyzed in the US, where populations have been meeting and mixing for hundreds of years, together with his co-authors in this paper highlights an important limitation of the study of the US patient cohort in underestimating the impact of racial diversity on ACLF outcomes (i.e., prevalence and severity of ACLF and risk factors of short-term mortality). The source dataset for the study of trends in mortality in patients with ACLF (defined according to the EASL-CLIF Consortium criteria) during the decade 2004–2014 in the US, precluded any further analysis of genetic ancestry and considered solely the information available on the US Department of Veterans Affairs Corporate Data Warehouse regarding reported race (i.e., 72.8% White vs. 17.2% African American) with 10% of the data for this variable not being available. It is worth noting that in the US patient cohort, African Americans were found to be more likely to develop ACLF but less likely to die within 28 days after hospitalization compared to reported Whites. Based on the results by the ACLARA study group, disparities regarding African Americans (reported race) could underlie the history of slavery and the trans-Atlantic slave trade that started in the 16th century and lasted until the 19th century with Africans carried to Brazil coming from Angola while those sent to North America, including the Caribbean, leaving from West Africa. This could explain, at least in part, why the reported percentage of African genetic ancestry in the US is of approximately 80% and in patients within ACLARA is approximately only of the 38%, with African ancestry being more prevalent in Brazil (17.9%) compared to other countries in the study.
The geographic distribution of admixture proportions in the ACLARA cohort is likely to be a reflection of the continuing impact of the demographic history on the genetic and racial diversity of populations across Latin America. It is remarkable that among the Latin American countries in the ACLARA study, Mexico showed the highest prevalence of severe ACLF among patients presented with ACLF at hospital admission followed by Chile, Colombia and Peru (65.3%, 63.3%, 58.4%, and 56.2%, respectively). Moreover, with the exception of the Colombian population which percentage of Native American ancestry was substantial and similar to that of Argentinians (31.8% and 32.8%, respectively), patients hospitalized in Peru, Mexico and Chile showed the highest percentages of Native American ancestry compared to the percentage of European genetic ancestry (82.8% vs. 14.8%, 63.9% vs. 30.6%, and 47.9% vs. 50.3%, respectively). Conversely, the percentage of European ancestry was higher in Brazil, Paraguay, Argentina, and Colombia (70.6%, 62.7%, 61.2%, and 54.6%, respectively).
The higher percentage of Native American ancestry seen in patients from Peru, Mexico and Chile within ACLARA is consistent with pre-history migration waves of the ancestors of the indigenous to the Americas arriving from northeast Asia, possibly across the Beringia land bridge or along the western coast of the Americas around 16,000 years ago. Moreover, European ancestry contributed the higher percentage of the overall genetic makeup of patients from Brazil, Paraguay, Argentina and Colombia which is also consistent with the arrival of the first European settlers from the Iberian Peninsula (Spaniards and Portuguese) during the 15th and 16th centuries and since the 19th century, migrations from Italy, Spain, Portugal, Germany and France, including Jewish communities from Central and Eastern Europe may have continued to contribute to the genetic admixture observed in modern Latin American populations.
"The study has practical implications. The conclusions highlight the impact of genetic ancestry, race and health care system access disparities on ACLF outcome. This information should be taken into account for management of patients (for example, granting priority of liver transplantation), improving public health policies in the region and dealing with recent internal migrations of people with those different backgrounds. Moreover, the region contains the Amazon rainforest, which is spread over huge extensions of land mass of many countries and populated mainly by Native Americans, found to be more vulnerable to ACLF. A closer look to those people is welcomed", concludes Flair Carrilho, co-lead investigator of the study and Principal Investigator at Hospital das Clínicas, University of São Paulo School of Medicine, Brazil.
This study was promoted by the European Foundation for the Study of Chronic Failure (EF CLIF).
Other authors on the study are Patrícia Momoyo Zitelli, Gustavo Pereira, Luciana L. Goncalves, Aldo Torre, Juan Manuel Diaz, Adrian C. Gadano, Angelo Z. Mattos, Liliana S.C. Mendes, Mario R. Alvares-da-Silva, Paulo L. Bittencourt, Carlos Benitez, Claudia Alves Couto, Manuel Mendizabal, Claudio L. Toledo, Daniel F. Mazo, Mauricio Castillo Barradas, Eva M. Uson Raposo, P. Martín Padilla-Machaca, Adelina Zarela Lozano Miranda, René Malé-Velázquez, André Castro Lyra, Milagros B. Dávalos-Moscol, Jose L. Pérez Hernandez, Rafael O. Ximenes, Giovanni Faria Silva, Oscar A. Beltrán-Galvis, María S. González Huezo, Fernando Bessone, Tarciso D.S. Rocha, Eduardo Fassio, Carlos Terra, Juan I. Marín, Patricia Sierra Casas, Carlos de la Peña-Ramirez, Ferran Aguilar Parera, Flavia Fernandes, Maria da Penha Zago-Gomes, Osvely Méndez-Guerrero, Sebastián Marciano, Angelo A. Mattos, Joao C. Oliveira, Gabriel T.S. Guerreiro, Liana Codes, Marco Arrese, Mateus J. Nardelli, Marcelo O. Silva, Renato Palma-Fernandez, Camila Alcantara, Cristina Sánchez Garrido, Jonel Trebicka, Thierry Gustot, Javier Fernández, Joan Clària, Rajiv Jalan, Paolo Angeli, Vicente Arroyo, and ACLARA study collaborators.
Publication information
Farias, A.Q.; Curto Vilalta, A.; Momoyo Zitelli, P.; Pereira, G.; Goncalves, L.L.; Torre, A.; Diaz, J.M.; Gadano, A.C.; Mattos, A.Z.; Mendes, L.S.C.; Alvares-da-Silva, M.R.; Bittencourt, P.L.; Benitez, C.; Alves Couto, C.; Mendizabal, M.; Toledo, C.L.; Mazo, D.F.; Castillo Barradas, M.; Uson Raposo, E.M.; Martín Padilla-Machaca, P.; Zarela Lozano Miranda, A.; Malé-Velázquez, R.; Castro Lyra, A.; Dávalos-Moscol, M.B.; Pérez Hernandez, J.L.; Ximenes, R.O.; Faria Silva, G.; Beltrán-Galvis, O.A.; González Huezo, M.S.; Bessone, F.; Rocha, T.D.S.; Fassio, E.; Terra, C.; Marín, J.I.; Sierra Casas, P.; de la Peña-Ramirez, C.; Aguilar Parera, F.; Fernandes, F.; da Penha Zago-Gomes, M.; Méndez-Guerrero, O.; Marciano, S.; Mattos, A.A.; Oliveira, J.C.; Guerreiro, G.T.S.; Codes, L.; Arrese, M.; Nardelli, M.J.; Silva, M.O.; Palma-Fernandez, R.; Alcantara, C.; Sánchez Garrido, C.; Trebicka, J.; Gustot, T.; Fernández, J.; Clària, J.; Jalan, R.; Angeli, P.; Arroyo, V.; Moreau, R.; Carrilho, F.J.; and ACLARA study collaborators. Genetic ancestry, race, and severity of acutely decompensated cirrhosis in Latin America. Gastroenterology 2023. DOI: 10.1053/j.gastro.2023.05.033
About EF CLIF
The European Foundation for the Study of Chronic Liver Failure (EF CLIF) is a private non-profit organization connecting biomedical researchers and healthcare professionals with each other, with patients and patient associations, and with society. The fundamental purpose of EF CLIF, reflected in its founding Statements of 2015, is to advance knowledge and promote research and education in liver disease to improve the prognosis of patients living with chronic liver failure.
The Foundation has made pioneering efforts in conducting a series of large, international prospective studies that have been instrumental in reclassifying the trajectory of patients with chronic liver failure and led to the clinical, prognostic and pathophysiological definition of the syndrome referred to as “acute-on-chronic liver failure” characterized by acute decompensation of cirrhosis, severe systemic inflammation, organ failures, and high short-term mortality. We are inspiring best clinical practices for the management of patients with chronic liver failure and promoting a more sustainable and equitable healthcare system.
Within the EF CLIF, the European Association for the Study of the Liver (EASL) Chair supports research activities through the EASL-CLIF Consortium, a network of 117 tertiary care and university hospitals in 28 European countries. The Grifols Chair promotes translational studies in centers across Europe and North America within the framework of the European Network for Translational Research (ENTR) with 21 centers in 7 countries. Over the last five years, EF CLIF has successfully expanded its geographical scope providing the context to support transcontinental collaborative research projects. The Global Projects chapter, which includes 96 centers in 22 countries, provides the framework to promote research in cirrhosis across the world with the aim to help to build consensus and ensure health equity worldwide.
ACLARA Study Collaborators
Caroline Marcondes Ferreira, Debora R. Benedita Terrabuio, Roberto M. Fernandes da Costa, Izabelle Venturini Signorelli, Caroline A. Pinto, Alma Estanes-Hernández, Jesús Ruiz Manriquez, María N. Gutierrez-Acevedo, Agustina M. Martinez-Garmendia, M. Ligia Aparecida, Everton Macêdo, Augusto Mantovani, Larisse Longo, Eduardo Garcia Vilela, María G. Valderrama, Michelle V.S. Santos-Rondon, Bertha Cardenas, Jorge Garavito Rentería, Lilian Montserrat Torres-Made, Laura C. Tenorio Castillo, José M. Aquino Ramos, María de Fátima Higuera de la Tijera, Rodrigo S. Aires, Diana C. Salinas-Gómez, Francisca Allendes, Fernando C. Schacher, Guilherme John Neto, Raúl Castro Valdivia, Josefina Pagés, Juan P. Roblero, Hugo Fainboim, Fernanda Fernandes Souza, Luis Colombato, Renata de Mello Peres, Larissa O. Miranda, Jade C. Oliveira, Leyla Nazal Ortiz, Daniela Simian, Gabriel Mezzano Puentes, Rita de Cássia Martins Alves da Silva, Iaarah Montalvo Gordon, Luis A. Chi Cervera, Marcos A. Girala Salomón, María T. Cuevas, Pedro Montes, y Máximo J. Cattaneo Buteler.