Acutely decompensated cirrhosis, which is a universally accepted condition, refers to the recent development of ascites, encephalopathy, gastrointestinal hemorrhage, or any combination of these disorders, in patients with cirrhosis. Acutely decompensated cirrhosis has been shown to be the most frequent cause of non-elective hospital admission among patients with cirrhosis. A large prospective observational agnostic European study (the CANONIC study) identified acute-on-chronic liver failure (ACLF) as a distinct syndrome among patients with acutely decompensated cirrhosis. ACLF was identified as the most severe form of acutely decompensated cirrhosis, characterized by intense acute systemic inflammation, the presence of hepatic failure, extrahepatic organ failures, or both, and a high risk of short-term death (i.e., death without liver transplantation within 28 days after hospital admission). Among European patients non-electively admitted for acutely decompensated cirrhosis, 30% either presented with ACLF or presented without ACLF but developed ACLF during the days or weeks after admission, whereas the remaining 70% were free of ACLF at presentation and remained free of ACLF within 28 days and had a very low short-term mortality. These “ACLF-free” patients also had less intense systemic inflammation than seen among those with ACLF. The prevalence of ongoing clinically apparent proinflammatory precipitants (mainly bacterial sepsis, alcoholic hepatitis, or both) was higher among patients with ACLF than among those without.
In the United States, racial minorities are disproportionately affected by acute infectious inflammatory diseases such as sepsis and COVID-19. The prevalence and severity of bacterial sepsis are higher among African American than among European American population. Moreover, a study examining population differences in the immune response to pathogens showed that African ancestry is associated with a stronger inflammatory response to pathogens than European ancestry. The rate of hospitalization for COVID-19 is higher among non-Hispanic Black persons, Hispanic or Latino persons, and non-Hispanic American Indian or Alaska native persons than among non-Hispanic White persons. In the United Kingdom, Black and South Asian people are at higher risk of COVID-19-related death than white people. In contrast, whether there are genetic ancestry- or race-related differences in health outcomes (ACLF, short-term death) have yet to be investigated in depth among patients with acutely decompensated cirrhosis.
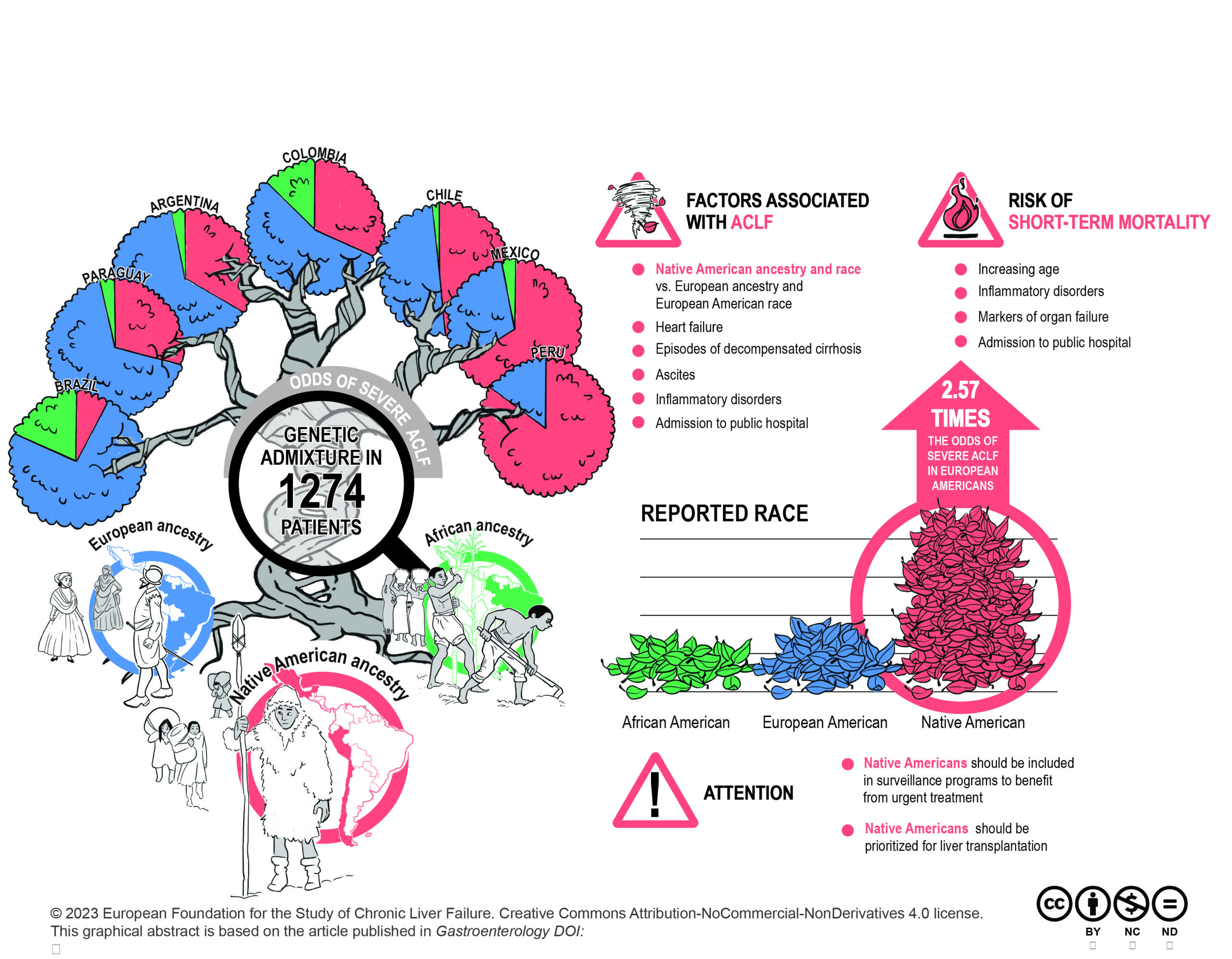
ACLARA was the first large prospective observational investigation of patients non-electively admitted for acutely decompensated cirrhosis to 44 hospitals from 7 countries in Latin America. The ACLARA study was conducted in Latin America because different races, including European Americans, African Americans, Native Americans and mixed races, are living in this continent. The ACLARA study was unique because it collected a comprehensive set of data. Indeed, not only the patients’ race was reported but also DNA was collected to assess the individual distribution of each of the three major genetic ancestries (i.e., European, African, and Native American). In addition, the ACLARA study collected sociodemographic characteristics, comorbidities, information on treatments administered before enrollment, and prior history of cirrhosis; clinical and laboratory data at enrollment; and outcomes within 28 days (including liver transplantation and death among non-transplanted patients). Therefore, the data obtained in the ACLARA study enabled us to construct multivariable models with the objective to assess whether differences in genetic ancestry or race are associated with ACLF at enrollment and short-term death among patients non-electively admitted to the hospital for acutely decompensated cirrhosis.
Of the 1274 patients, 395 (31.0%) had ACLF of any grade at enrollment. As compared with patients without ACLF, those with ACLF had significantly higher median percentage of Native American genetic ancestry and lower median percentage of European ancestry, were more frequently of Native American race and less frequently of European American race. The median percentage of African genetic ancestry and the percentage of patients of African American race did not differ between the ACLF and no-ACLF groups. Native American genetic ancestry and Native American race were also overrepresented among patients with severe ACLF (ACLF-2 or -3) relative to patients with ACLF-1. In multivariable analyses, higher percentage of Native American genetic ancestry and Native American race (vs. European American race) were independently associated with increased odds of ACLF of any grade at enrollment, after adjustment for differences in sociodemographic and clinical characteristics. Overall, 66 (5.2%) patients underwent liver transplantation and 243 (19.1%) died without transplantation. As compared with patients who survived, those who died were significantly older, had significantly higher median percentage of Native American genetic ancestry and lower median percentage of European genetic ancestry. The median percentage of African genetic ancestry did not significantly differ between the two groups. A significantly higher percentage of patients who died than patients who survived were Native Americans. A significantly lower percentage of patients who died than patients who survived were European Americans or African Americans. In adjusted time-to-event analyses, neither genetic ancestry nor race was associated with the risk of short-term death. Variables that were associated with higher short-term mortality were increasing age, admission to public hospital (vs. private hospital), and enrollment with proven bacterial infection and sepsis, or alcohol-related hepatitis; lower arterial pressure or lower SpO2 to FiO2 ratio; higher blood levels of creatinine, or international normalized ratio; lower blood levels of albumin; or higher white blood cell counts.
The main objective of this project was to investigate the association of a variety of factors, including genetic ancestry, race, sociodemographic factors, etiology of cirrhosis, ongoing treatments, with ACLF at presentation and short-term death in a large population of Latin American patients non-electively admitted to the hospital for acutely decompensated cirrhosis. The most striking novel finding of this study was that Native American genetic ancestry or Native American race (vs. European American race) were independently associated with ACLF at presentation, finding that indicate differences in genetic ancestry or race contribute to outcome disparities in cirrhosis. The association of Native American genetic ancestry and Native American race with ACLF indicate that Native American patients with cirrhosis should be included in programs of tight surveillance in order to benefit from urgent treatment of triggers of acute decompensation of liver disease. This could be first step toward precision medicine, which is an unmet medical need in the field of decompensated cirrhosis. In addition, the discovery that differences in genetic ancestry and race are associated with differences in outcomes among patients with acutely decompensated cirrhosis, may change the policy of prioritization and allocation of liver transplants in these patients.
Richard Moreau, Principal Investigator

European Foundation for the Study of
Chronic Liver Failure
Avinguda Diagonal 477, 11th floor
08036 Barcelona, Spain
Tel: +34 93 227 14 00
Email: Send us an email
© 2025 European Foundation for the Study of Chronic Liver Failure
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |